Looking for up-to-date information on asthma? You can find it here!
We’ve linked resources from multiple providers into one place so it’s easy for you to find what you need.

New guidelines for asthma management were published in 2020. Along with incorporating recent advances in the treatment of asthma, they recognise the inequities in asthma care experienced by Māori and Pacific peoples. Pharmacist prescriber Helen Cant outlines what has changed in guideline recommendations and, in collaboration with medical writer Gayle Robins, discusses strategies for reducing the disproportionate asthma burden in Māori and Pacific peoples.
After reading this article it is expected you will be able to:
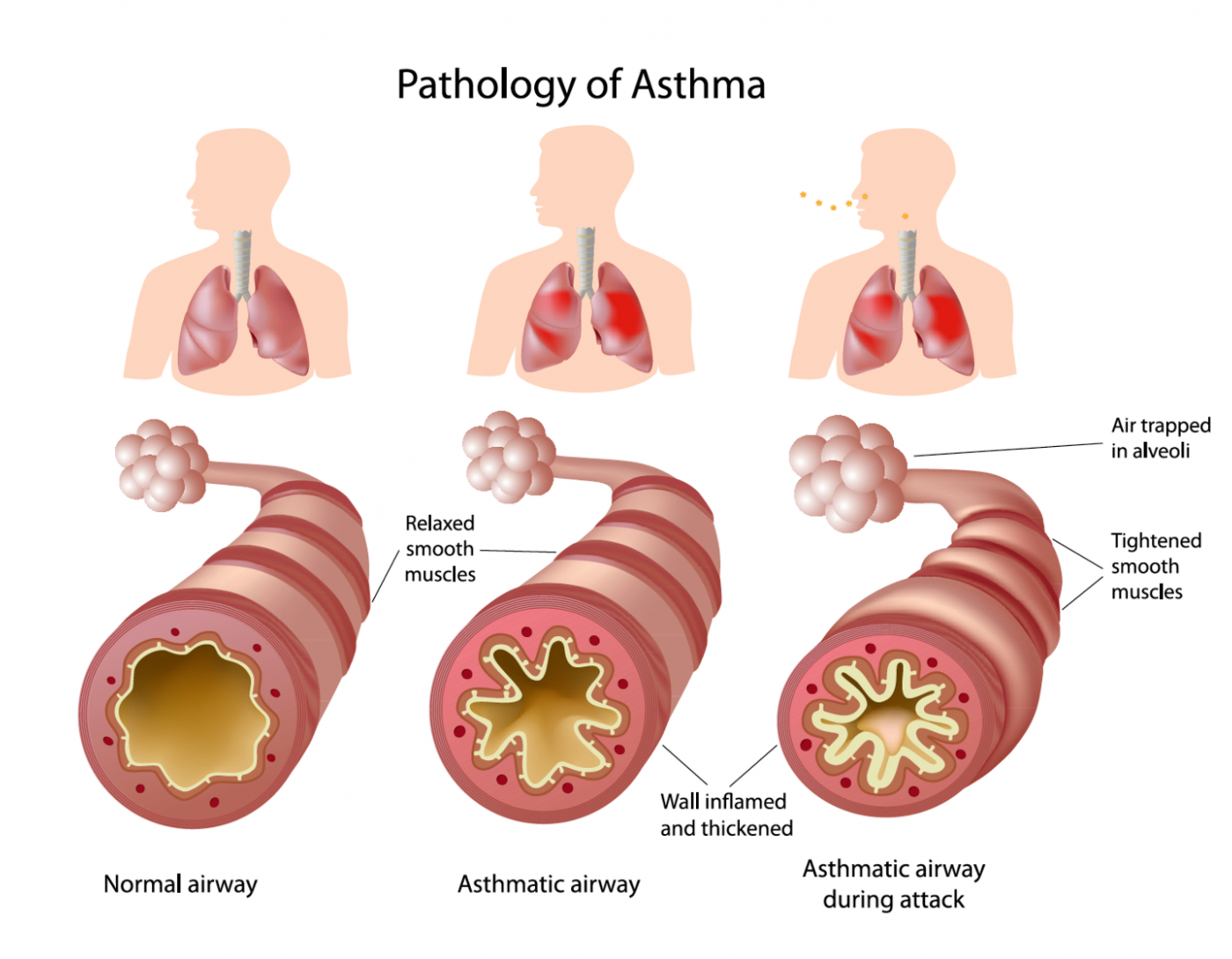
Asthma is characterised by a reversible narrowing of the airways due to tightening of muscle in the wall of the airway, and by inflammation and swelling of airway mucosa (Panel 1). Airway narrowing and excess mucus production lead to a variety of symptoms and signs including wheezing, cough, shortness of breath and observed breathing difficulty.
Asthma is a major public health problem in New Zealand affecting up to 20 per cent of children and adults. According to a recent report, the prevalence of asthma in New Zealand has not significantly changed over the years 2000 through 2019 and asthma hospitalisations have even declined slightly. Mortality rates, though, while reaching a low point in 2010 have increased, hitting a high point in 2017 of 2.5 deaths per 100,000 people in New Zealand.1
Although overall asthma prevalence has stayed generally static, this is not the case for Māori and Pacific peoples, where asthma remains more prevalent than in non-Māori, non-Pacific peoples, and hospitalisation and death due to asthma are unacceptably high – disparities that have been persistent in New Zealand for years now.1
In 2019, asthma hospitalisations for both Māori and Pacific peoples were more than three times those of New Zealand Europeans (rate ratios 3.24 and 3.22, respectively), with the ratio for Māori increasing markedly from that reported in 2018. Asthma mortality rate ratios over 2012–2017 followed the same pattern: respectively, Māori and Pacific peoples had rates 3.36 and 2.76 times those of New Zealand Europeans.1
Despite awareness of these differences, the level of care Māori and Pacific peoples receive does not match their disease burden. And, for a number of years, studies have documented disparities in the two main aspects of asthma management, namely:2
Māori with asthma are less likely to be prescribed inhaled corticosteroids (ICS), have an action plan or receive adequate education, in addition to facing other major barriers to good asthma management such as poor access to care, and services that do not meet their needs. These considerations are likely to be similar in Pacific peoples.3 Education, knowledge and self-management help to reduce disparities and need to be an ongoing component of asthma care, along with appropriate medication.
Asthma is caused by a combination of genetic and environmental factors. For many people, it occurs in combination with allergic conditions, such as eczema or allergic rhinitis (hay fever), or they may have relatives with these conditions.
There are different types of asthma, but the underlying airway narrowing is a result of:
Symptoms – wheezing, shortness of breath, cough, chest tightness, difficulty breathing out and increased mucus production.
Triggers – infections, allergens (eg, pollen, dust mites, pets), smoke, exercise, weather (eg, cold or humidity), chemicals (eg, perfumes, cleaning products, aerosol sprays) and stress.
Medicines, such as beta-blockers (including in eye drops), NSAIDs and aspirin, can also trigger asthma. NSAIDs and aspirin can often be taken safely as they do not trigger asthma in everyone.
ACE inhibitors frequently cause a cough that can be confused with asthma, and in some people with unstable airways, these drugs may trigger an asthma attack.
People should be encouraged to identify their asthma triggers.
People with well-controlled asthma:
Effective self-management of asthma requires patients and their whānau to have a good understanding of asthma and how it is managed. People who are unaware of what good asthma management looks like are more likely to normalise and accept sub-optimal asthma control. Healthcare professionals have a valuable role in improving this understanding, supporting patients/whānau and improving outcomes by embedding asthma education into their practice.4
Asthma education should be tailored to the patient/whānau. Poor asthma literacy is associated with reduced self-efficacy and decreased use of asthma medicines and is likely to contribute to asthma disparities. Always ensure asthma information is communicated in a way that aligns with patient/whānau health literacy, and check for understanding.4 The Health Quality and Safety Commission’s “Three steps to meeting health literacy needs” has been developed in the context of achieving equitable health outcomes for Māori and maintaining cultural safety. It provides a useful framework for assessing patient/whānau asthma knowledge, allowing existing information to be reinforced and gaps in understanding or misconceptions to be corrected.
Once a patient’s level of asthma knowledge has been established, it can be built on step by step – with a focus on expanding one aspect in the understanding of asthma at every point of contact.4
When in discussion with patients be sure to use appropriate language, not jargon, and try to adopt terms the patient or their whānau has used, thereby building a common language. For example, use “puffer” if the patient refers to their inhaler in this way. Avoid overloading patients with too much information at a time – start with the most important point. Be creative when trying to increase understanding – use illustrative analogies, and “what-if” scenarios where patients describe how they would manage a situation likely to result in asthma.
Offer targeted resources for patients to take away; check with asthma service providers for availability of these. A map providing a directory of local asthma societies with contact details is available from the Asthma and Respiratory Foundation NZ. ARFNZ has a variety of asthma resources, with some offered in te reo Māori, and in Samoan, Tongan and Chinese languages.
Everybody with asthma should be encouraged to have a personalised asthma action plan. These provide direction to patients on when and how to adjust treatment over the short term in response to worsening symptoms, and when to access additional medical care. They have been shown to improve health outcomes and reduce hospitalisations.3,4 Plans should be updated annually, and be appropriate for treatment level, asthma severity, health literacy, culture and self-management ability.
Action plans come in a range of formats – written, pictorial, electronic, app – with adult and child asthma action plans available in te reo Māori, Samoan, Tongan and English. They can be downloaded from the ARFNZ website, ordered in print and are available on the My Asthma App (see Asthma resources at the end of this article). The foundation also provides adult asthma action plans as interactive PDFs; these can be customised by the health professional and emailed to the patient.
Action plans may be based on symptoms with or without peak flow measurements and are either three or four-stage depending on both patient and health professional preference. The four-stage plan has an extra step giving patients the option of increasing the dose of ICS up to four-fold, by increasing the frequency of use and/or the dose.3
Asthma management is a cycle of ongoing assessment, treatment and review. Remember, when discussing asthma management with patients/whānau, personal goals should be included and documented as shared goals of care.
New asthma guidelines were published by the ARFNZ in 2020 and include recommendations for improving care in Māori and Pacific peoples.3 There are no longer separate guidelines for adults and adolescents (people aged 12 and over) as treatment is the same. The child guidelines have also been reviewed and updated.5 These guidelines are based on recommendations by the Global Initiative for Asthma (GINA).
The GINA Assembly includes members from 45 countries. Every year, they publish a report6 and a pocket guide,7 with the intent to provide a comprehensive international approach to management of asthma and to provide clear guidelines and feasible tools for clinical practice, using a strong evidence base.
In 2019/20, there were major changes to GINA’s recommendations for asthma treatment. The large, double-blind study used to support the GINA recommendations investigated AIR/SMART therapy: the combined inhaled corticosteroid (ICS)/fast onset long-acting beta2 agonist (LABA) budesonide/formoterol, used either as needed or regularly plus as needed.
It is important to note that these recommendations apply only to people with asthma, not to people with chronic obstructive pulmonary disease (COPD).
Previous recommendations date back many years and were based on the belief that mild asthma was primarily bronchoconstriction. We now know that inflammation of the airways is found in most people with asthma, even if they only have symptoms intermittently.
Clinical studies have shown that treatment with an ICS significantly reduces the frequency and severity of asthma symptoms, and markedly reduces the risk of experiencing, or even dying from, an asthma attack.
Strong evidence shows that, although short-term relief of asthma is achieved with short-acting beta2 agonist (SABA)-only treatment, this does not protect from severe exacerbations. In fact, regular or frequent use of SABA treatment increases the risk of exacerbations, worsening airway inflammation and lung function, and increasing allergic reaction.
The GINA report states that overuse of SABA treatment (eg, three or more canisters per year) is associated with an increased risk of severe exacerbations, and 12 or more canisters per year is associated with increased risk of asthma-related death.6
The new recommendations aim to:
Anti-inflammatory reliever (AIR) therapy is the use of a combination budesonide/formoterol inhaler as a reliever medication. It can be used either only as needed, or regularly plus as needed. This approach includes and extends the “single combination ICS/LABA inhaler maintenance and reliever therapy” (SMART) approach previously recommended. The AIR regimen and the use of asthma action plans have been shown to improve outcomes for Māori.3
AIR therapy in New Zealand – the only ICS/fast-onset LABA combination currently available in New Zealand is budesonide/formoterol, and only the dry powder inhalers are approved for reliever use. A budesonide/formoterol pressurised metered dose inhaler is available, but using it this way would represent an off-label prescription.
Starting asthma treatment with a SABA (ie, salbutamol or terbutaline) alone is no longer recommended. Instead, it is recommended an ICS be initiated from first diagnosis.
This can be done either by introducing AIR treatment or by using traditional ICS/SABA therapy (see later). One of the risks of traditional ICS/SABA therapy is that people do not use the ICS and rely solely on the SABA. AIR therapy removes this risk as the ICS is included in the reliever treatment as well as maintenance treatment.
The stepwise approach to asthma management entails a patient stepping up management levels as required to achieve and maintain asthma control and reduce exacerbation risk. A step down is considered if symptoms are controlled for three months and the patient is at low exacerbation risk.3
Step 1 – one inhalation as required to relieve symptoms to a maximum of six inhalations on a single occasion or a total of up to 12 inhalations daily.8 This results in a similar short-term bronchodilator response to that of a 200µg dose (ie, two 100µg doses) of salbutamol and, in adults and adolescents with mild asthma, reduces the risk of a severe asthma exacerbation by at least 60 per cent compared with SABA reliever alone.
Step 2 – regular maintenance treatment is implemented as either one inhalation twice daily or two inhalations once daily, depending on patient preference. Plus one inhalation as required, to a maximum of six inhalations on a single occasion or a total of up to 12 inhalations daily.8
Step 3 – maintenance treatment is stepped up to two inhalations twice daily. Plus one inhalation as required, to a maximum of six inhalations on a single occasion or a total of up to 12 inhalations daily.8
In adults and adolescents taking maintenance ICS/LABA therapy, budesonide/formoterol used as a reliever reduces the risk of a severe asthma exacerbation by about one-third compared with using a SABA reliever. Thus, budesonide/formoterol used both as a reliever plus regularly as maintenance therapy is the preferred treatment for patients with moderate to severe asthma.
The current recommendations are:3
Step 1 – introduce standard-dose ICS as maintenance treatment, plus a SABA as needed.
Step 2 – use standard-dose ICS/LABA as maintenance treatment, plus a SABA as needed.
Step 3 – use high-dose ICS/LABA as maintenance treatment, plus a SABA as needed.
Note the recommendation that if a severe exacerbation of asthma occurs, consider switching to AIR therapy.
ICS doses
For most people, most of the clinical benefit is obtained with low-dose ICS. Some people will need standard-dose ICS if their asthma is not well controlled with low-dose ICS, but concordance and inhaler technique should be checked first. A few will need high-dose ICS.
When an ICS is initiated as maintenance therapy together with a SABA reliever, a standard dose of ICS should be used. The recommended standard daily doses of the different ICS preparations for adults are3:
*Subsidised brands at time of publishing
Additional treatments for asthma may include:
Long-acting muscarinic antagonists – are not subsidised in New Zealand for the treatment of asthma, although tiotropium is Medsafe-approved for add-on maintenance treatment. Note that LAMAs are funded for patients with COPD, and there will be a significant cohort who have coexisting asthma and COPD.
Montelukast – is a leukotriene receptor antagonist. In New Zealand, it is indicated for adults and children over the age of two for prophylaxis of asthma or relief of allergic rhinitis (seasonal or perennial). Montelukast should be considered as add-on therapy when control is not achieved with optimal standard treatment; for everyone with respiratory conditions exacerbated by aspirin; and may be useful in exercise-induced asthma or in people with coexisting rhinitis.3
Note the precaution around neuropsychiatric side effects with montelukast.9 Patients taking this medicine should be advised to contact a health professional if they experience sleeping problems, unusual dreams, changes in behaviour, hallucinations, anxiousness or agitation, confusion or suicidal thoughts.10
Mast cell stabilisers – sodium cromoglicate and nedocromil inhalers are approved for use in mild asthma; however, the supplier, Sanofi, has discontinued supply in New Zealand and these inhalers are no longer available. Patients should be managed on alternative treatments, in line with current asthma guidelines.11
Other treatments – include oral corticosteroids, theophylline, azithromycin and monoclonal antibodies, many of which will only be used following specialist review.
The New Zealand Child Asthma Guidelines were updated in June 2020.5 As well as prescribing recommendations, these guidelines include important ways that all health professionals can help children with asthma (see Panel 2).
The guidelines also summarise the medication approaches for children of different ages (see later). The goal is for all children to use an inhaler device that is appropriate for their development, including consideration of whether a spacer or mask is appropriate.
It is important that children’s treatment includes regular review to allow step-up or step-down through treatment options as appropriate for symptom control.
Children aged one to four years – who wheeze are considered in a different way from children aged five to 11, as many preschool children with post viral wheeze do not have asthma or do not go on to develop asthma.
The current recommendations are:5
Step 1 – SABA reliever alone (one to two puffs when needed)
Step 2 – add maintenance low-dose ICS
Step 3 – add montelukast
Step 4 – refer to a paediatrician.
Note that if SABA, ICS and montelukast are insufficient, Step 4 is referral to a paediatrician. This means that LABAs are not part of the routine management of wheeze or asthma in this age group.
Children aged five to 11 years – assessment of inhaler technique and adherence to treatment remains key in this age group.
The current recommendations are:5
Step 1 – SABA reliever alone (one to two puffs when needed)
Step 2 – add maintenance low-dose ICS
Step 3 – add LABA
Step 4 – increase to standard dose of maintenance ICS/LABA; add montelukast; consider referral to a paediatrician
Step 5 – consider high-dose ICS/LABA; refer to a paediatrician.
At Step 5, the child will likely be having frequent oral steroids and should definitely be referred to a paediatrician.
Currently, there is insufficient evidence to recommend SMART as first-line therapy in children aged 11 years and younger. However, SMART using budesonide/formoterol 100µg/6µg may be considered on specialist advice in select children aged five to 11 years, who are poorly controlled at Steps 3 to 5.
|
Ambulance
|
Influenza vaccine
|
|
Relationships
|
Access
|
|
Smoke exposure
|
Concordance
|
|
Housing
|
Asthma action plan
|
|
Income
|
Health literacy
|
Source: New Zealand Child Asthma Guidelines
Asthma attacks can be very serious, even fatal. They are more common and more severe in people with poorly controlled asthma and in high-risk people, but they can occur in anyone with asthma. High use of SABA inhalers indicates poor asthma control and increases the risk of severe exacerbation and mortality.
Many people will still be using SABA-only treatment for mild asthma. In 2018, over two million salbutamol inhaler devices were dispensed in the community setting in New Zealand,12 making it the eighth most dispensed Pharmac-funded medicine.13
It is worth asking people how much SABA they are actually using – inhalers tend to get lost or given to someone else, and some people will want to have inhalers in different rooms of the house, or in the car or sports bag, for example.
Also be aware that many people on ICS/SABA therapy don’t collect their ICS prescriptions, and may rely on high doses of SABA to relieve symptoms. AIR/SMART therapy may be beneficial for these people as having one combined ICS/LABA inhaler for as-needed use, and for regular use if required, not only ensures that the ICS is taken more regularly but also provides safer treatment right from the start.
Another important reminder is that people with asthma should continue taking all prescribed asthma medications during the ongoing COVID-19 pandemic.
Worldwide, it is estimated that up to 80 per cent of people do not use their inhaler correctly, and at least 50 per cent do not use their maintenance medications as prescribed.7 Inhaler technique remains critical to optimal therapy, no matter which inhaler device is being used.
Inadequate technique is among the most common reasons, along with poor adherence, for sub-optimal asthma control,3 so it is a good idea to routinely check patient technique at each visit. Remember, always ensure good technique before initiating any increase in treatment.
Patients can access videos on correct inhaler technique via on the National Asthma Council Australia website. If a patient has persistent difficulty with their technique, consider switching to an alternative inhaler device. The UK’s National Institute for Clinical Excellence has a patient inhaler decision aid that contains information to help adults with asthma, and their healthcare professionals, when discussing options for inhaler devices.
People who use a metered-dose inhaler may benefit from administering their dose with a spacer as many will find it challenging to coordinate their inhaler use with their breathing. Spacers help deliver the medicine directly into the lungs, rather than the mouth and throat, thus markedly increasing medicine effectiveness. Spacers also reduce local side effects from ICS inhalers such as hoarseness, throat irritation and oral candidiasis – but remind patients to still rinse their mouth after ICS use.
Spacers should be supplied free of charge to patients; they can be ordered, fully subsidised, on a Practitioners Supply Order. Instruct patients to wash spacers weekly with warm water and detergent, and to let them air dry to reduce static charge.
All health professionals have a role in improving health outcomes and health equity as well as delivering high quality, effective asthma care. Ways for health professionals and services to achieve this include:2-4
Research has shown that appropriately designed and delivered health programmes improve Māori health outcomes.2 Leadership from Māori is needed in developing asthma management programmes that improve access and enable “wrap around” services targeting the wider barriers Māori face in asthma care.3
These barriers include cost and affordability of care, poor access to care and poor quality or discontinuous care, services or approaches not meeting needs, culturally inappropriate services, institutional racism, lack of trust and confidence in the health system, unhealthy indoor environments in high deprivation areas, and increased risk factors such as obesity and smoking.3
Systemic changes will be required to address these wider barriers to care for Māori and Pacific peoples. A paradigm shift is under way with New Zealand’s health reforms. The role of the newly formed partnership between Te Aka Whai Ora – Māori Health Authority, Te Whatu Ora – Health New Zealand, and Manatū Hauora – Ministry of Health is to lead and monitor transformational change in the way the entire health system understands and responds to the health and wellbeing needs of Māori and their whānau. A central tenet is ensuring everyone has the same opportunities to achieve good health outcomes by creating a fairer, more coordinated and connected health system. It is long overdue.
Helen Cant is a pharmacist prescriber working in general practices in Tokoroa.
Gayle Robins is a freelance medical writer and regular contributor to He Ako Hiringa resources.
Pharmacists - a set of CLASS reflection activities and peer group guides has been prepared in relation to this article, to help you meet your Pharmacy Council annual recertification requirements - download here.
GPs and nurses - you may also find the CLASS activities useful, or you may wish to just complete the self-assessment questions, which you can find in the 'CLASSact answer template' here.
This activity has been endorsed by The Royal New Zealand College of General Practitioners (RNZCGP) and has been approved for up to 0.5 CME credits for continuing professional development purposes (1 credit per learning hour). To claim your CPD credits, log in to your Te Whanake dashboard and record these activities under the appropriate learning category.
This activity has been endorsed by the PSNZ as suitable for inclusion in a pharmacist’s CE records for CPD purposes.
![]()


Looking for up-to-date information on asthma? You can find it here!
We’ve linked resources from multiple providers into one place so it’s easy for you to find what you need.